Leishman Stain Composition: Benefits And Procedure

The Leishman stain composition involves a precise blend of chemicals that selectively stain different components of blood cells. The main …
The Leishman stain composition involves a precise blend of chemicals that selectively stain different components of blood cells. The main …
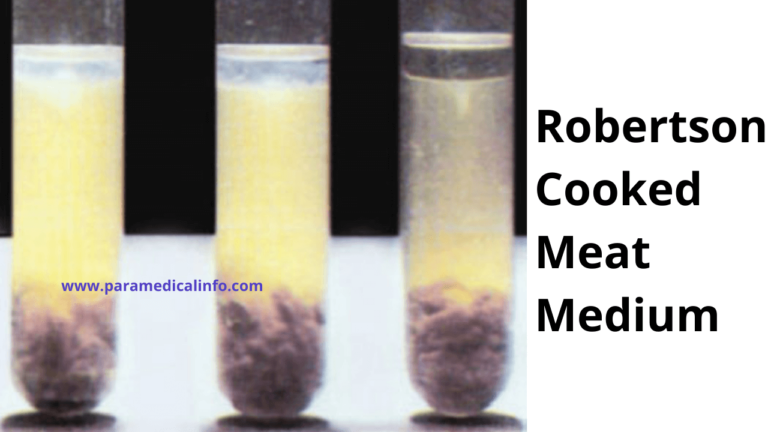
Robertson Cooked Meat Medium is an excellent medium for the primary growth and maintenance of aerobic and anaerobic organisms. Robertson …
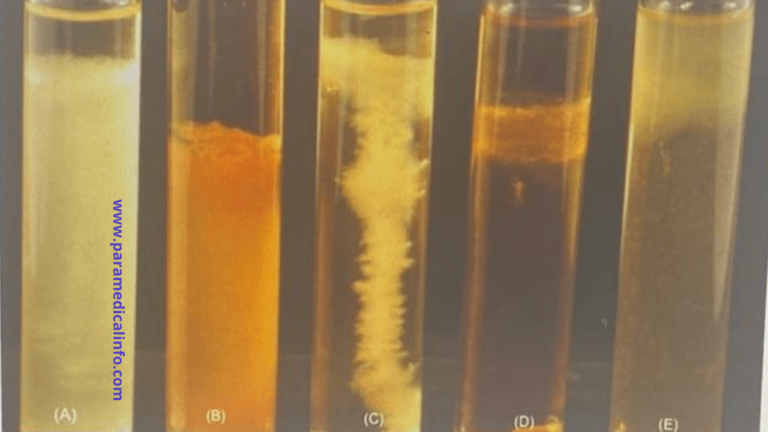
Fluid Thioglycollate Medium (FTM) is used for the isolation and cultivation of aerobic and anaerobic organisms and is widely used …
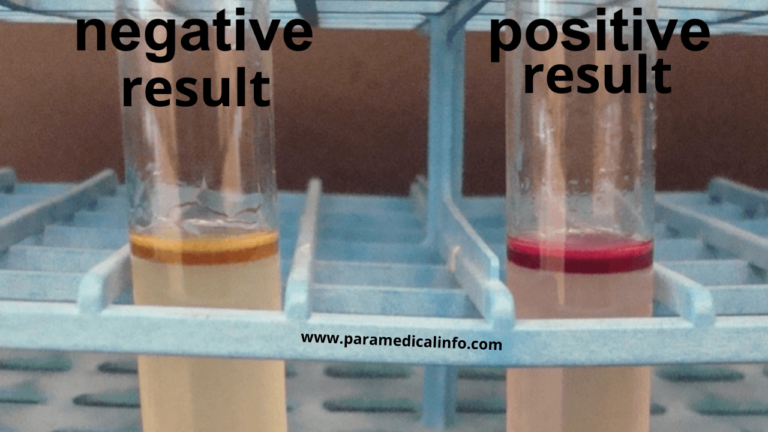
Kovacs Reagent Preparation first dissolves para-dimethylamino benzaldehyde in normal amyl alcohol. Slowly add Hydrochloric Acid—store at 4°C. To test for …
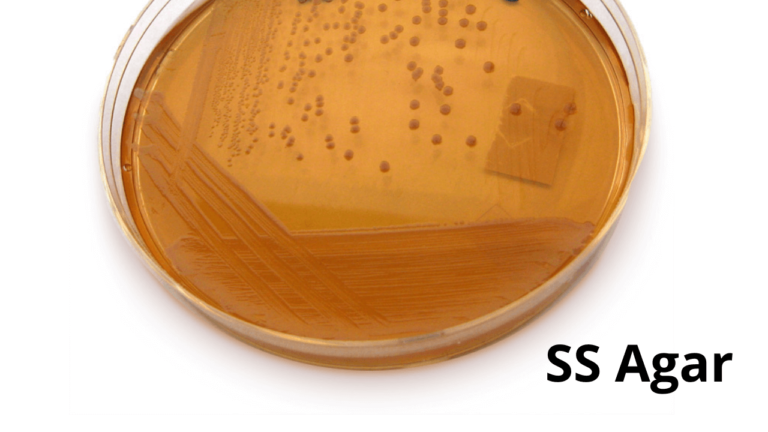
SS Agar (Salmonella Shigella Agar) is a differential selective media used for the isolation of Salmonella and some Shigella species …